Nicotine, the Wonder Drug

Nicotine delivery devices like the patch could offer surprising benefits to people diagnosed with certain neurological disorders. Cristina Pedrazzini/Science Photo Library.
This notorious stimulant may enhance learning and help treat Parkinson’s, schizophrenia and other neurological diseases.
Every drug of addiction must have its day. Morphine remains one of the most potent painkillers ever discovered. Cocaine’s chemical cousin lidocaine is still used by physicians and dentists as an effective local anesthetic. Even demon alcohol, when taken in moderation, cuts the risk of heart attacks, osteoporosis, rheumatoid arthritis and a hodgepodge of other ailments.
Now comes nicotine, perhaps the most unlikely wonder drug ever to be reviled.
If dozens of human and animal studies published over the past six years are borne out by large clinical trials, nicotine — freed at last of its noxious host, tobacco, and delivered instead by chewing gum or transdermal patch — may prove to be a weirdly, improbably effective drug for relieving or preventing a variety of neurological disorders, including Parkinson’s disease, mild cognitive impairment (MCI), Tourette’s and schizophrenia. It might even improve attention and focus enough to qualify as a cognitive enhancer. And, oh yeah, it’s long been associated with weight loss, with few known safety risks. (Although, in truth, few safety studies of the increasingly popular e-cigarettes have yet been published.)
Nicotine? Yes, nicotine.
In fact, the one purpose for which nicotine has proven futile is the very same one for which it’s approved by the Food and Drug Administration, sold by pharmacies over the counter, bought by consumers and covered by many state Medicaid programs: quitting smoking. In January 2012, a six-year follow-up study of 787 adults who had recently quit smoking found that those who used nicotine replacement therapy in the form of a patch, gum, inhaler or nasal spray had the same long-term relapse rate as those who did not use the products. Heavy smokers who tried to quit without the benefit of counseling were actually twice as likely to relapse if they used a nicotine replacement product.
And therein lies the conundrum that physicians and regulators will have to wrestle with if the promising studies about nicotine’s benefits hold up: how to endorse a drug linked to one of the greatest public health scourges the world has ever known.
“I understand that smoking is bad,” says neuroscientist Maryka Quik, program director of the Neurodegenerative Diseases Program at SRI International, a nonprofit research institute based in California’s Silicon Valley. “My father died of lung cancer. I totally get it.”
Yet over the years, she has published dozens of studies revealing the beneficial actions of nicotine within the mammalian brain. “The whole problem with nicotine is that it happens to be found in cigarettes,” she says. “People can’t disassociate the two in their minds.”
Tweaking the Brain
The first hint of nicotine’s curious benefits came from a study published in 1966 by Harold Kahn, an epidemiologist at the National Institutes of Health. Using health insurance data on 293,658 veterans who had served in the U.S. military between 1917 and 1940, Kahn found the kinds of associations between smoking and mortality that had already become well known. At any given age, cigarette smokers were 11 times as likely to have died of lung cancer as nonsmokers, and 12 times as likely to have died of emphysema. Cancers of the mouth, pharynx, esophagus, larynx — on and on. But amid the lineup of usual suspects, one oddball jumped out: Death due to Parkinson’s disease occurred at least three times as often in nonsmokers as in smokers.
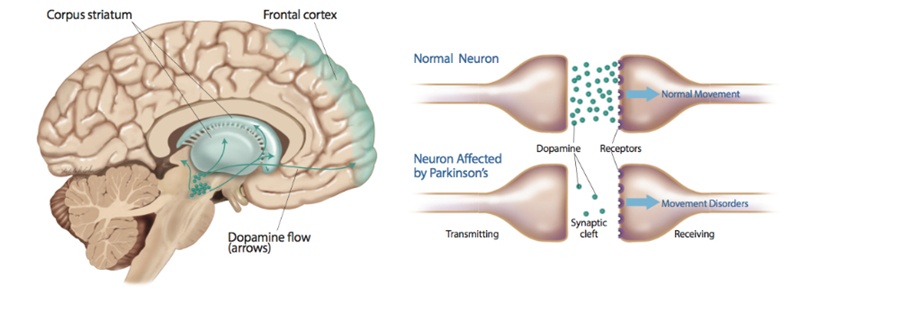
The neurotransmitter dopamine sends signals related to pleasure, reward and motor function across neurons in the brain. A lack of dopamine has been linked to movement disorders such as Parkinson’s disease. ©2013 Delilah R. Cohn
Following up, researchers expected the finding to be just a statistical aberration in Kahn’s data, but instead quickly confirmed it. Grasping at a final possible alternative to the inconvenient notion that smoking could have a healthful benefit, experts theorized that the association was due only to smokers dying young of cancer, heart disease and lung disease before the age when they might otherwise have developed Parkinson’s. (The neurodegenerative disorder affects about 1 percent of people by age 60, rising to about 4 percent by age 80.) But in 1971, epidemiologists Irving Kessler and Earl Diamond of Johns Hopkins University published a study comparing the smoking history of living Baltimore residents recently diagnosed with Parkinson’s with age-matched controls. Sure enough, they found that the Parkinson’s patients were much less likely than other residents to have ever smoked.
So what was it about tobacco that ravaged the heart, lungs, teeth and skin but somehow guarded against a disease of the brain? In 1979, UCLA neurobiologist Marie-Françoise Chesselet showed that nicotine increases levels of dopamine, a neurotransmitter essential for boosting attention, reward-seeking behaviors and risk of addictions, from gambling to drugs. Dopamine also helps control movement. Nicotine receptors in the striatum, the comma-shaped structure near the center of the brain where movements are planned and controlled, are located near the terminals that regulate and emit dopamine. Even a small dose of nicotine, Chesselet found, stimulates the release of dopamine in the striatum, putting the brakes on movement that otherwise would go uncontrolled.
And that effect suggests why nicotine could help treat Parkinson’s disease. Called “the shaking palsy” in an 1817 essay by the English physician James Parkinson (after whom the disease was later renamed), Parkinson’s is marked by shaking and difficulty with walking, coordination and all other movements. Although its ultimate cause remains unexplained, neuroscientists have long known that as symptoms worsen, dopamine-producing neurons in the striatum die out. Since the 1960s, the gold-standard treatment for the disease has been the drug levodopa, also known as L-dopa, a dopamine precursor that can cross the blood-brain barrier. But the drug is not perfect: L-dopa treatment eventually induces dyskinesia — quick, involuntary movements of the hands, and sometimes of the head and trunk.
Putting together the emerging lines of evidence, Quik decided to treat Parkinson’s disease in squirrel monkeys by administering nicotine. In a landmark 2007 paper, she reported that the monkeys had 50 percent fewer tremors and tics, and that nicotine had reduced dyskinesia 35 percent in those already receiving L-dopa. Studies by Quik and others involving rats, mice and nonhuman primates have since found similar effects. In short, by driving dopamine, nicotine appeared to ease the tremors and tics caused by Parkinson’s, and even the movement disorder induced by the major Parkinson’s drug.
Waiting for Human Evidence
Given the findings, one might reasonably ask how many clinical trials of ordinary over-the-counter nicotine patches or gum as a preventative for the progression of Parkinson’s have been published in the medical literature. “In humans, none,” says neurologist James Boyd of the University of Vermont College of Medicine. That will change soon. Boyd is now running two such studies. The first, begun in 2010, is a small, randomized 12-week trial of whether a nicotine patch can reduce another problem often associated with Parkinson’s: impulsivity.
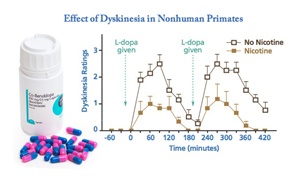
A 2007 study suggests that nicotine treatment could help alleviate the dyskinesia often experienced by Parkinson’s patients being treated with L-dopa (left). Chart: Allison Mackey/Discover after Quick, et al. “Nicotine and Parkinson’s Disease: Implications for Therapy.”
Remember, Parkinson’s involves a loss of dopamine, a neurotransmitter that regulates not only movement but also addictive behaviors. It has long been observed that people who develop Parkinson’s tend to be more low-key and risk-averse than average, as if their innate dopamine levels have always been on the low side. When they take L-dopa, however, some have been known to swing to the other side of the reward-seeking spectrum, developing gambling or sexual addictions. Boyd hopes nicotine might push such patients back to a middle ground.
He is also the principal U.S. investigator for a randomized trial that began late last year in Germany and is now being conducted here to test the value of nicotine as a therapeutic drug. The study seeks to answer whether ordinary over-the-counter nicotine gum or patches can halt the progression of Parkinson’s. To get at the answer, one component the study will look at is whether the chemical can relieve the writhing, twisting movements that eventually beset almost every Parkinson’s patient taking L-dopa.
Beyond Parkinson’s
While researchers await the results of the Parkinson’s studies, they look beyond to nicotine treatments for other disorders as well.
“Nicotine has separate mechanisms by which it may protect brain cells, aside from its influence on dopamine,” Boyd says. “One of the functions of nicotinic receptors is to moderate the entry of calcium into cells. The presence of nicotine increases the amount of intracellular calcium, which appears to improve cellular survival.”
And nicotine may have an antioxidant effect, serving to mop up the toxic free radicals produced as a byproduct of metabolism, thus protecting the brain. The neuroprotective effects of nicotine were studied in a randomized clinical trial involving 67 subjects in the early stages of Alzheimer’s disease, where memory was slightly impaired but decision-making and other cognitive abilities remained intact. They received either a 15-milligram nicotine patch or placebo for six months. The results found “significant nicotine-associated improvements in attention, memory and psychomotor speed,” with excellent safety and tolerability.
Other studies suggest that nicotine may be as effective at enhancing attention as methylphenidate (Ritalin) and the wakefulness-promoting drug modafinil (Provigil). In 2008, Paul Newhouse, director of the Center for Cognitive Medicine at Vanderbilt University School of Medicine in Nashville, compared performance on a series of cognitive tasks in 15 nonsmoking ADHD patients while wearing either a 7-mg nicotine patch or a placebo patch. After just 45 minutes with the nicotine patch, the young adults were significantly better at inhibiting an impulse, delaying a reward and remembering an image they had seen.
Even people without any diagnosed disorder might benefit from nicotine. Psychologist Jennifer Rusted of the University of Sussex in Britain calls the drug “the most reliable cognitive enhancer that we currently have.” In addition to improving visual attention and working memory, nicotine has been shown by Rusted to increase prospective memory: the ability to remember and implement a prior intention. (When your mother asks you to pick up a jar of pickles at the grocery store on the way home, she’s saddling you with a prospective memory challenge.)
“It’s a small effect, maybe a 15 percent improvement,” Rusted says. “It’s not something that’s going to have a massive impact in a healthy young individual. But we think it’s doing it by allowing you to redeploy your attention more rapidly.” In short, the drug seems to work by helping users shut out irrelevant stimuli so that important information can come to the fore.
The ability to shut out stimuli could also turn nicotine into a treatment for schizophrenia, where afflicted individuals are overwhelmed by sights, sounds and thoughts that most of us would either ignore or quickly dismiss. Studies in the United States, Canada and Germany have shown that nicotine improves the ability of people with schizophrenia to focus their attention and recall recent events. In addition, the potent antipsychotic haloperidol often causes dyskinesia, which Quik’s 2007 study proved nicotine can relieve.
Not the Great Satan
Perhaps most surprising is that, in studies by Boyd and others, nicotine has not caused addiction or withdrawal when used to treat disease. These findings fly in the face of nicotine’s reputation as one of the most addictive substances known, but it’s a reputation built on myth. Tobacco may well be as addictive as heroin, as some have claimed. But as scientists know, getting mice or other animals hooked on nicotine alone is dauntingly difficult. As a 2007 paper in the journal Neuropharmacology put it: “Tobacco use has one of the highest rates of addiction of any abused drug.” Paradoxically it’s almost impossible to get laboratory animals hooked on pure nicotine, though it has a mildly pleasant effect.
The same study found that tobacco smoke itself is necessary to amp up nicotine’s addictiveness. In 2005, for instance, researchers at the University of California, Irvine, found that animals self-administer a combination of nicotine and acetaldehyde, an organic chemical found in tobacco, significantly more often than either chemical alone. In 2009, a French team found that combining nicotine with a cocktail of five other chemicals found in tobacco — anabasine, nornicotine, anatabine, cotinine and myosmine — significantly increased rats’ hyperactivity and self-administration of the mix compared with nicotine alone.
In short, the estimated 45.3 million people, or 19.3 percent of all adults, in the United States who still smoke are not nicotine fiends. They’re nicotine-anabasine-nornicotine-anatabine-cotinine-myosmine-acetaldehyde-and-who-knows-what-else fiends. It is tobacco, with its thousands of chemical constituents, that rightly merits our fear and loathing as the Great Satan of addictiveness. Nicotine, alone: not so much.
Despite the potential benefits and apparent safety, researchers like Boyd want more evidence before they’ll recommend a nicotine patch for anything other than its FDA-approved (but seemingly useless) purpose, smoking cessation. “Nicotine has potential drug interactions. It can interfere with blood pressure medications. To recommend something for which there is no good long-term safety data — it’s just wrong,” Boyd says.
To Quik, the upside is clear. “People have tested all their favorites to help treat Parkinson’s and other neurological disease,” she says. “Now nicotine’s time has come.”
[This article originally appeared in print as “The Nicotine Fix.”]
(This article was originally published online, in 2014, here.)